
Real-wold
Evidence & Economics
Evidence - Intermountain Healthcare
83% of nurses recommended the adoption of MedLite ID.
78% of nurses reported increased overall patient safety and care.
81% of nurses noticed improved efficiency associated with line tracing.
87% of nurses claimed reduced stress associated with line tracing.
Evidence - Utah Tech
100% decreased the time it took them to find the medication line with an overall time savings of 34%, or nearly one minute.
100% expressed how the MedLite ID reduced their stress levels.
Average time savings per trial was 57.3 seconds with just 4 lines.
51% nursing productivity/ efficiency improvement.
Evidence - MedLite Tape Study
80% of the used rolls tested positive for pathogens.
16 of the 36 bacteria and fungi found were pathogenic.
Two bacteria identified as critical or serious by the World Health Organization.
Evidence - Peer Review Published Study
The study in the Journal of Infusion Nursing conducted at Wake Forest University School of Medicine found:
Six out of eight errors occurred in low-light conditions, which are common in ICU conditions. MedLite ID has zero errors in low-light conditions.
24% percent faster in accessing the primary medication line injection port
40% less mental tasking as quantified within the study.
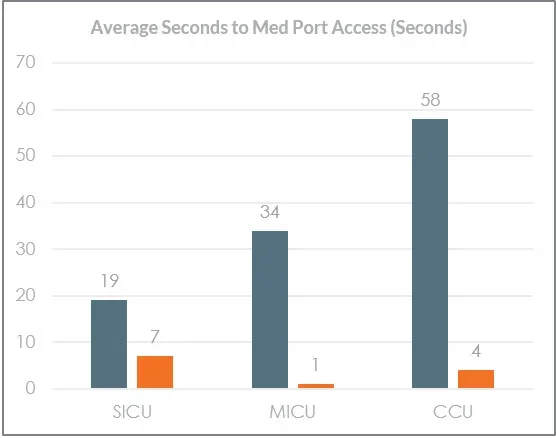
Evidence - Patient Trial, 500 Bed Veteran Affair Hospital
CCU, MICU, SICU / 1 month baseline data, 3 months product trial data
Standard of Care (Tape/Labels): 19-58 seconds, time to access primary medication line port
MedLite ID: 1-7 seconds, time to access primary medication line port
271%+ improvement from MedLite ID
MedLite Evidence Summary
83% Nurse Adoption
What Can MedLite Smart Lites Do For You?
✔ 78% Increase in Patient Safety
✔ 34% Reduction in Time to Identify
✔ 81% Improved Efficency
✔ 87% Nurse Stress Reduction
✔. 200% reduction in time to access port
Best Practices for multiple IV co-administration infusions.
From AHRQ: An Inadvertent Bolus of Norepinephrine. Administration of multiple IV infusions is ubiquitous in the ICU, and there are several established safety parameters associated with medication concentration, dosing, and pump programming. The physical dexterity required for administering multiple IV infusions concurrently is underappreciated, and lack thereof can, in fact, lead to serious harm. AHRQ addressed this issue in a recent article, including recognizing risks associated with medication administration, the most frequent types of IV medical errors in the ICU, and best practices for the co-administration of multiple IV infusions. (Reprinted with permission.)

Eligible for AMA PRA Category 1 Credit and
Maintenance of Certification Part II credit
MedLite ID & Infectious Disease
Healthcare workers can be exposed more often due to numerous infected individuals. Reducing the frequency and intensity of exposure to infectious diseases list MRSA or SARs-CoV-2 might reduce the infectious dose and result in less severe cases.
MedLite ID takes a minutes procedure and turns it into seconds to identify and trace key infusion lines. Doing that every 1-2 hours for multiple patients adds up. The ability to identify key infusion lines and reduce exposure protects both the patient and nurse alike. MedLite can also be used with extension tubing to further reduce exposure.
Reduce exposure to infectious disease by up to two hours per day per 12-hour shift. Not marketing math, simple math...

Economics

What is the cost of doing nothing?
Based on literature rates of infusion wrong-route ADE, a 100-bed hospital is projected to be at-risk for 22 infusion ADEs annually.
This is an annual loss of $450K in direct costs and unplanned inpatient days.
After paying for MedLite ID, a net $244K in savings is possible.
nfusion ADE Impact
For Every 100 Beds of Hospital
Adding MedLite ID converts a daily loss to a daily savings
✔ 56% of ADEs are Infusion Related
✔ 19 ADEs per 1000 ICU Patient Days
✔ 17+ Drugs Per Day in ICU
✔ $6600 Average ADE Costs Per Event
✔ 15% of Infusion ADE = Wrong Route Errors
✔ Cost/day of $2883 of each unplanned inpatient day
✔ Average medical malpractice claim $242K
✔ 2% risk of Mortality from ADE